Output from both Government and Media on Covid19 has been characterised by confusion and hysteria. People are genuinely afraid,
partly because they are deprived of the information needed to do some rational thinking. Central to this is the U.K. Government’s Chief Adviser on Epidemiology, Prof. Neil Ferguson of Imperial College, London. While Ferguson is considered an “expert” in these matters, other experts disagree with him, and his work has attracted massive criticism. First and foremost, the model he is using to make his predictions is not open to other scientists. Openness and the formal process called “Peer Review” are essential to science. Without that transparency, anything he says should be disregarded. Except, perhaps, his statement to the Financial Times that “We don’t have a clear exit strategy at the moment.” That is the Government’s top scientific adviser speaking. The only good news here is that, even though Ferguson doesn’t know the way out, others do
Epidemiology
The basics of Epidemiology are obviously known to Epidemiologists. Now is the time for some of that to be understood by others. The science is not that difficult to follow.
In Epidemiology there is a basic, well recognised model called the SIR (Susceptible, Infectious, Resistant) Model. Ferguson knows this, but his version of the model is wrapped up in “thousands of lines” of code which he does not publish. Other Epidemiologists manage to do their calculations on an ordinary Spreadsheet that anyone else can then check. Essentially the model divides a population into those three categories with respect to any virus.
Herd immunity can be easily understood from the SIR Model. Herd immunity is achieved when a sufficient proportion of any given population is immune. This immunity may be arrived at through vaccination, or, especially in the absence of a vaccine, it may be arrived at through contact with the disease. Because of the Government confusion and Media hysteria, people imagine that this means most of the population ending up in ICU, and possibly dying to achieve herd immunity. The truth is that huge numbers of people will become infected and gain immunity without ever having symptoms. Others will think they had a cold. All of us can think of an occasion when a family member had an unpleasant illness, but others in close contact “didn’t catch it.” In fact, they often did, and they became immune, but they never noticed. There is no evidence to suggest that Covid19 is any different; indeed, rather the reverse. Even from a personal anecdotal viewpoint, I was recently in Spain for a month, coincidentally flying back just as lockdown began there. I knew two children, in different parts of Spain, who had classic Covid19 symptoms. One of them didn’t even take to her bed. My wife and I both had very funny “colds” that we remember extremely well, because they threatened the timing of a long journey we had planned within Spain. We are certain all four were Covid19 cases, but none of the many other contacts from family, restaurant meals, etc showed any symptoms. Most must have been infected, and therefore become immune. The point here is that building herd immunity through exposure is not a notably dangerous process.
The Graph below is a SIR Model graph. It is not nearly as complex as it may first appear. It is taken with gratitude from work by Prof. Knut Wittkowski. (More details in references below, including a note on his status.) What it shows is the progress of a virus epidemic (such as COVID 19) in a population of ten million people.
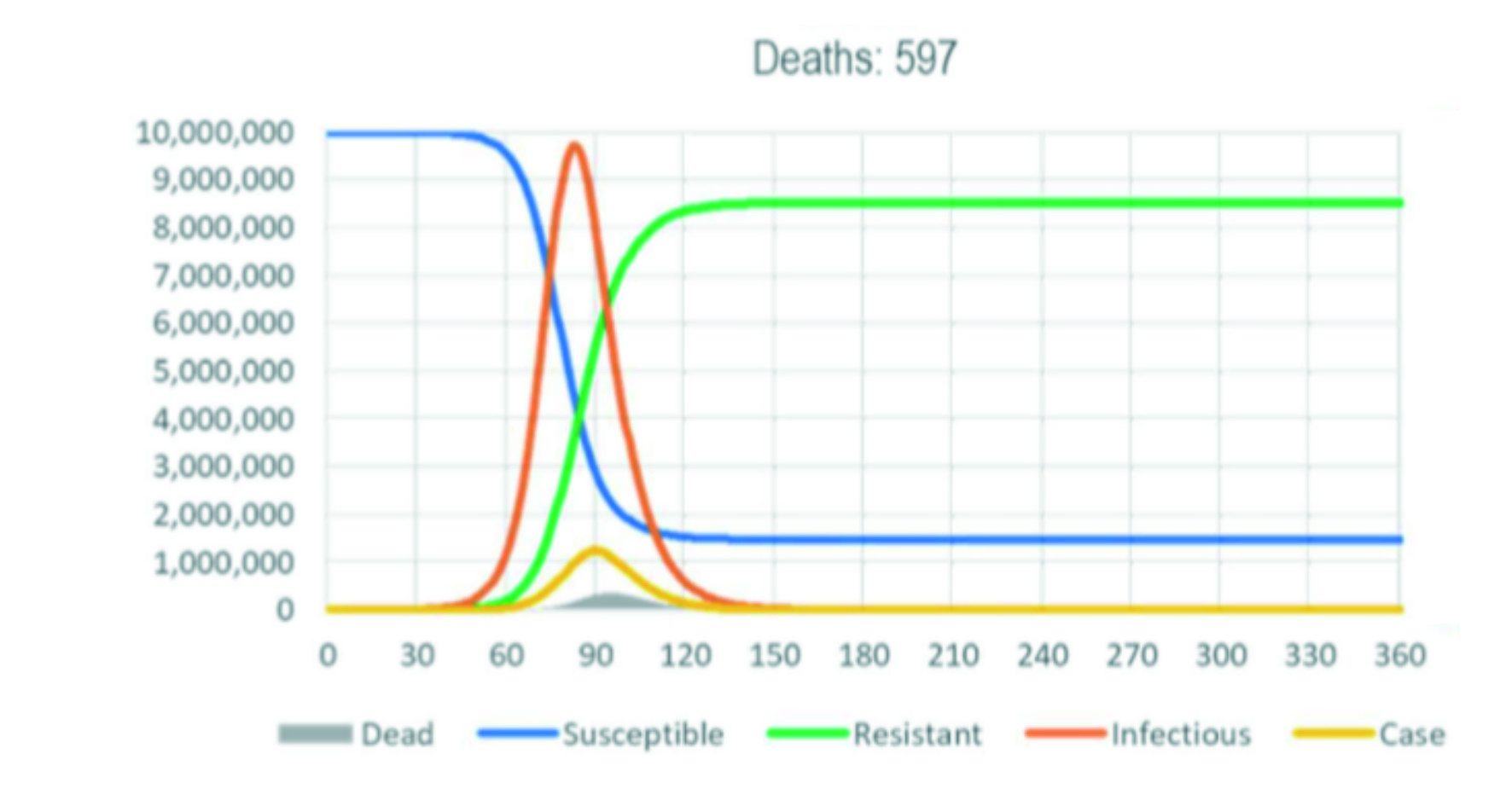
Points to note are the red line, which shows people who are infected and infectious. This number of people rises very rapidly to a peak, then falls away just as rapidly. An important parameter is the basic reproduction number R0 (pronounced R nought). It is the number of people an infectious person entering a fully susceptible population would infect through direct contact. Under the assumption of a basic reproduction number of 2.2, it takes only about two weeks from the first cases being recognized (yellow line) to the peak of the number of infectious people (red line). The blue line represents people who are susceptible to the disease. To begin with, this is everybody; notice that on the left the line starts at 10 million, the whole population. As the epidemic progresses the number of people who are susceptible rapidly decreases. As they become immune, they join the R-for-Resistant group shown by the green line. As the green line moves upward an infectious person meets fewer and fewer susceptible people, which is why the number of new infections (red line) goes down. When the Resistant group makes up about 80% of the population herd immunity is achieved, and the epidemic is over. The yellow line shows actual cases observed. These are people with serious symptoms. Notice how much lower that number is compared with all those infected. And at the very bottom is the grey line, showing those who died. (The red, yellow and grey lines are shown on an arbitrary scale to be visible.)
What the Science Shows
The case shown in the graph is one where there is no intervention by Government. The fear with no intervention, as we are constantly reminded, is that the NHS may be overwhelmed. Given that the NHS has been cut to the bone for so long, that fear is understandable. But the key issue here is at what point in the epidemic the lockdown begins. In China, it naturally took some time for them to know what they were dealing with. How do you pick out a novel Upper Respiratory Infection from among all the other Upper Respiratory Infections that are doing the rounds? Especially during winter, which is the season for such things? By the time the Chinese were able to react to the epidemic, it was already well advanced, therefore the number of infections had already begun to decline because many people were already immune. The supposed result of the lockdown was actually the natural decline of infections, because most of the work of building immunity had already occurred naturally.
We have the opposite problem in the UK. Here, the lockdown started too soon. The Government was initially planning to let herd immunity develop, but lost its nerve in the face of some daunting projections. They jumped into full lockdown, which stopped, and continues to stop, the development of herd immunity. In this situation, the virus can go on causing infections and deaths for an extremely long period. They have, in effect, painted us all into a corner. There are still plenty of susceptible people, and plenty of virus around to infect them, and because of the hysteria, plenty of fear of doing anything different. Hence talk of even keeping the lockdown for months to wait for a vaccine that may never come. And in the meantime, pushing the economy into a crash that may be far worse than 2008.
The Way Forward
Fortunately, there is a way out, and it’s not difficult to understand. First, the aim of the lockdown is to “Save the NHS”. All we ever hear about the NHS is stories of nurses battling through exhaustion in packed wards to avert deaths. I’m very grateful to the Heath Service Journal, a subscription-only publication for top health service managers, for dropping their paywall so that anyone can see their information. Key facts we now know are that the huge, new 4,000 bed NHS Nightingale Facility in London, ten days after opening, only has 19 patients. And that acute beds across the NHS are 40% empty. This means there is scope to ease the lockdown, move the economy again, and increase immunity through contact, without overwhelming the hospitals.
And there is much more. The average death rate among cases is about 8%. That is a scary figure. Who wants an illness that gives you an almost 1 in 10 chance of dying? But if we cut through the hysteria, we find something rather different. Figures from Italy show that 90% of deaths were among people aged 65 or over, or who already had other illnesses (called comorbidity.) Office for National Statistics have just confirmed the same pattern in the UK. Moreover, only very few of the elderly had no comorbidities, so there is a big overlap in these two groups. Clearly high-risk individuals need to be shielded as much as possible. But the other side of the coin is that for healthy people aged under 65 the chance of death is only one tenth as great, namely 0.8% (and for children it is so low that they were initially considered to be naturally immune). That’s a big difference – it is comparable to a regular flu. The even bigger difference comes from the fact that the death figure is deaths among CONFIRMED cases. Looking back at the graph, you’ll see there’s a huge difference between getting infected and getting immune, and actually winding up with serious symptoms, to the point where you become a Confirmed Case. If we assume only 5% of all cases are ever confirmed (and it could well be less) then that death possibility for healthy under 65’s goes down to 0.04%. Most people won’t be able to relate to that figure; it’s somewhat higher than your whole lifetime probability of being struck by lightning.
All of the above leads to a very obvious way forward, which is what we should have done in the first place. We should shield the over 65’s and other vulnerable groups, and let everyone else get on with their lives. It just happens that in the UK the vulnerable people make up about 20% of the population, and they are also largely inactive economically. Locking them down therefore has a minimal effect on the economy. And the other 80% can go about their lives infecting each other, with minimal harm, until they are all immune, at which point herd immunity would be achieved. So then the over 65’s can be re-integrated with very little risk.
How is it that nobody else seems to know this? If you think back to the 2008 Financial Crash, everybody thought the Boom would go on forever, including all those who knew about economics. Yet anyone who knows economics also knows that Bust follows Boom like night follows day. But the then Chancellor, Gordon Brown, repeated the mantra that “The days of Boom and Bust are over.” And everybody went into “group-think”, which in reality is no thought at all. That is, everybody apart from a website called housepricecrash.co.uk. But they were ignored, because they were in a tiny minority. It is crucial to understand that science is not decided by politicians, by democratic vote, or by popular opinion, but solely by evidence and sound analysis.
Some good news today, 15th April. Denmark is reopening Primary Schools, joining the Swedes and Icelanders, who never closed them, (or shops or restaurants) and never suffered as a result. Austria and Spain are also relaxing. Germany has a scientific advisory board, the Leopoldina, that recommended to open schools “as fast as possible”. NHS Providers say “enough beds.” What we need now is for our own Government to also begin these take sensible actions. “Now” in this context meaning Now.
References:
Wittkowski Status. Rockefeller University have just released a statement saying that he was not a Professor there, although he never claimed to have been. They are splitting hairs. For twenty years Dr Wittkowski was Head of the Department of Biostatistics, Epidemiology, and Research Design there. From a layman’s perspective, that means working as a Professor. Further, he previously worked with Prof. Klaus Dietz at the University of Tubingen and became a Professor there. Dietz has been a key player in the development of the now fully accepted concept of R0 in Epidemiology.
Prof Ferguson, Exit Strategy. Financial Times. (You will need to register.) https://ftalphaville.ft.com/2020/04/04/1586015208000/Imperial-s-Neil-Ferguson—We-don-t-have-a-clear-exit-strategy-/
Prof Ferguson Lack of Transparency. Nature Magazine. About half-way down article it says he is “trying to tidy up code for release.” The article otherwise just provides more confusion. https://www.nature.com/articles/d41586-020-01003-6
For Epidemiology and SIR see Researchgate: https://www.researchgate.net/figure/Typical-SIR-model-solution-showing-progression-of-population-disease-states-for_fig1_224209140
Prof Knut Wittkowski. Go here: https://ratical.org/PerspectivesOnPandemic-II.html Click on Two Epidemics of Covid-19 at the top of the page for a pdf of article by Wittkowski, and scroll down the page for text of an interview with him.
Financial Crash. Guardian. Shows the usual ignorance of epidemiology, but understands the likely economic effects of the response. https://www.theguardian.com/business/2020/apr/08/the-2008-financial-crisis-will-be-seen-as-a-dry-run-for-covid-19-cataclysm
NHS Situation. Health Service Journal. Patients at London Nightingale: https://www.hsj.co.uk/service-design/exclusive-nightingale-largely-empty-as-icus-handle-surge/7027398.article
NHS Empty beds: https://www.hsj.co.uk/acute-care/nhs-hospitals-have-four-times-more-empty-beds-than-normal/7027392.article
General Statistics. https://www.worldometers.info/coronavirus/
Death by Age in Italy. Statista.com. https://www.statista.com/statistics/1105061/coronavirus-deaths-by-region-in-italy/
Death by Age in UK. BBC /ONS. https://www.bbc.co.uk/news/health-52308783
Probability of being struck by lightning. National Geographic. https://www.nationalgeographic.com/news/2005/6/flash-facts-about-lightning/ Others put the odds even lower, but at this level of probability it hardly matters.
© Copyright 2020 Keith Rushworth. The full article or its contents may be reproduced with acknowledgement if, and only if, such references properly and fully reflect the arguments stated.
With appreciation for advice in drafting this from Dr Knut Wittkowski.